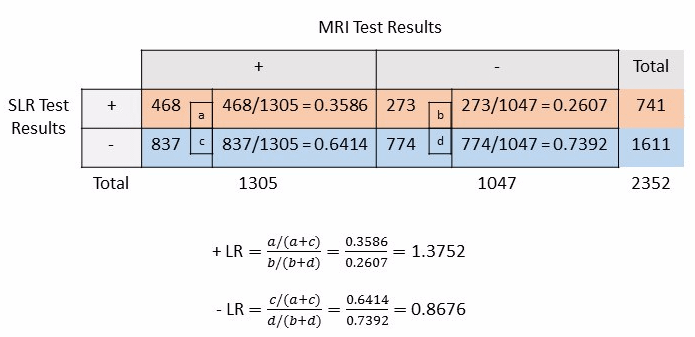
Let us continue using the data from the study by Capra et al (1).
The likelihood ratio is the percentage of diseased individuals with a given test result divided by the percentage of healthy individuals with the same test result (2).
The likelihood ratios (positive and negative) can be calculated by using the following formulae (2):
+ LR = sensitivity / (1- specificity)
= True positive rate / False positive rate
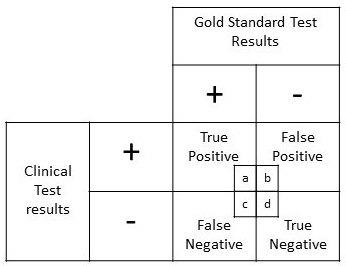
= [a/(a+c)] / [b/(b+d)]
= [TP/(TP+FN)] / [FP/(FP+TN)]
– LR = 1- sensitivity / specificity
= False negative rate / True negative rate
= [c/(a+c)] / [d/(b+d)]
= [FN/(TP+FN)] / [TN/(FP+TN)]
The likelihood ratio is an index of diagnostic accuracy that can help refine the clinical diagnosis on the basis of signs and symptoms, as they possess the following properties (3).
- Likelihood ratios (both positive and negative) are stable indices than sensitivity or specificity with changes in the disease prevalence.
- Likelihood ratios can be calculated for dichotomous as well as polychotomous test results.
- Likelihood ratios can be used to estimate post-test probability by hand calculation or by using Fagan’s nomogram for Bayes theorem (4) if pre-test probability is known.
The likelihood ratios (positive and negative) are calculated as follows:
Interpretation of LRs (5):
It is suggested that + LR of 10 or more is a statistical indication that the positive test is good at correctly diagnosing the disease.
Also, – LR of 0.1 or less is an indication that the negative test is good at correctly ruling out the disease.
And, LR of close to 1.0 will not provide much change in the probability of a person having or not having the disease.
References:
- Capra, F., Vanti, C., Donati, R., Tombetti, S., O’reilly, C. and Pillastrini, P., 2011. Validity of the straight-leg raise test for patients with sciatic pain with or without lumbar pain using magnetic resonance imaging results as a reference standard. Journal of manipulative and physiological therapeutics, 34(4), pp.231-238.
- Sackett, David L & Sackett, David L. Clinical epidemiology (1991). Clinical epidemiology: a basic science for clinical medicine (2nd ed). Little, Brown, Boston, MA
- Grimes, D.A. and Schulz, K.F., 2005. Refining clinical diagnosis with likelihood ratios. The Lancet, 365(9469), pp.1500-1505.
- Fagan TJ. Letter: nomogram for Bayes theorem. The New England journal of medicine. 1975;293(5):257.
- Davidson, Megan. “The interpretation of diagnostic tests: a primer for physiotherapists.” Australian Journal of Physiotherapy 48.3 (2002): 227-232.